Atrial Rhythms Flashcard
Rationale
D. Rationale: Atrial flutter is not the only atrial arrhythmia that produces the distinct sawtooth appearance on ECG. Paroxysmal atrial tachycardia with atrioventricular block is thought to be brought about by an ectopic focus originating in the atrium. It will have the distinct finding of a sawtooth appearance on ECG. This will be difficult to delineate with type 2 atrial flutter with a 2:1 atrioventricular block.
Answer choice A – A first-degree atrioventricular block manifests as a prolonged PR interval.
Answer choice B – Premature atrial beats will manifest as early beats lacking a resting phase between two beats.
Answer choice C – Torsade’s de pointes is a dysrhythmia caused by low serum magnesium levels and closely resembles ventricular fibrillation.
Question
An ECG characteristic described as a sawtooth appearance is seen in which one of the following cardiac arrhythmias?
a. First-degree atrioventricular block
b. Premature atrial beats
c. Torsade’s de pointes
d. Paroxysmal atrial tachycardia with atrioventricular block
Answer
d. Paroxysmal atrial tachycardia with atrioventricular block
Rationale
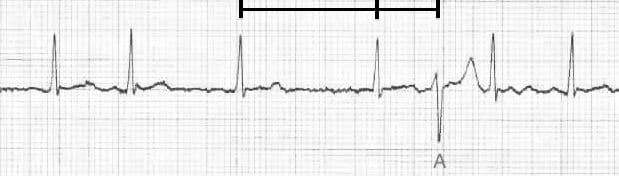
B. Rationale: The Ashman beat is an often isolated wide QRS complex seen in the presence of atrial fibrillation. It is observed when a premature supraventricular beat occurs before a right bundle-branch block has recovered from its refractory period (see ECG image below). The ‘A’ indicates the Ashman beat.
Answer choice A – A PVC is an early beat originating from an irritated focus within the ventricles.
Answer choice C – A bundle branch block is represented by a prolonged QRS complex as there is an electrical block preventing the normal spread of an electrical impulse throughout the ventricles.
Answer choice D – A PAC is an early beat originating from the atria. It appears normal but comes early and is followed by a compensatory pause.
Question
An ECG tracing that shows an abnormally long R-R interval followed by a QRS complex with an rSr’ configuration without any compensatory pause is brought about by which aberration in atrial fibrillation?
a. Premature ventricular contraction
b. Ashman beat
c. Bundle branch block
d. Premature atrial contraction
Answer
b. Ashman beat
Rationale
C. Rationale: The ECG above represents fibrillatory waves characteristic of atrial fibrillation. Atrial fibrillation is brought about by fibrosis in the atrial myocardium, overloading of the atria due to untreated hypertension, and cardiomyopathy, to name a few. In the example above, this ECG was obtained from a patient without any definite pathology.
Answer choice A – A third-degree AV block would manifest as complete AV dissociation, meaning there would be no correlation between where the P waves and QRS complexes fall.
Answer choice B – Atrial flutter manifests as a rhythm with a characteristic sawtooth pattern.
Answer choice D – Atrioventricular is a type of supraventricular ventricular tachycardia but does not manifest as fibrillatory waves characteristic of atrial fibrillation.
Question
Refer to the ECG tracing below from a 61-year-old woman with no subjective complaints. Which one of the following cardiac arrhythmias produces this ECG finding?

a. Third-degree atrioventricular block
b. Atrial flutter
c. Atrial fibrillation
d. Atrioventricular nodal re-entrant tachycardia
Answer
c. Atrial fibrillation
Rationale
A. Rationale: Impulses originating above the ventricles have QRS complexes < 0.12 seconds. If impulses originate below the AV node, the QRS complex is widened and prolonged (> 0.12 seconds). Also, impulses originating in the atria (rather than the SA node) present with abnormal P wave morphology: P waves may be flattened, notched, peaked, or have a saw-tooth appearance.
Question
Which of the following findings are distinct for arrhythmias that are atrial in origin?
a. QRS complex < 0.12 seconds
b. PR interval 0.12–0.2 seconds
c. Irregular R-R intervals
d. All of the abovementioned findings represent arrhythmias originating in the atria
Answer
a. QRS complex < 0.12 seconds
Rationale
B. Rationale: This is atrial tachycardia. It has all the morphologic findings of a premature atrial contraction, but it occurs throughout the ECG strip. The P waves vary in morphology (see arrows) and may be buried within the T wave.
Question
Which of the following rhythms is caused by an irritable focus within the atria that has overcome the sinoatrial node. The rate is 150–250 bpm, and the rhythm is regular, with a P wave morphology that varies and may sometimes be buried within the T wave, a PR interval of 0.12 seconds, and a QRS complex < 0.12 seconds?

a. Premature atrial contraction
b. Atrial tachycardia
c. Supraventricular tachycardia
d. Atrial flutter
Answer
b. Atrial tachycardia
Rationale
B. Rationale: Atrial tachycardia is caused by an intensely irritable focus in the atria. It causes a very fast rate > 250 bpm, with a characteristic saw-tooth appearance because of the cyclic pattern of generated impulses creating atrial waves. The PR interval cannot be measured because it is indistinguishable in the ECG strip. The QRS complex is normal.
Question
Which one of the following arrhythmias is produced by an intensely irritable focus causing a rate > 250 bpm with a saw-tooth appearance due to the cyclic pattern of impulse generation creating a series of atrial waves?

a. Wandering pacemaker
b. Atrial tachycardia
c. Atrial flutter
d. Atrial fibrillation
Answer
b. Atrial tachycardia
Rationale
B. Rationale: Atrial fibrillation is caused by an intensely irritable focus that shows barely visible fibrillatory waves within the isoelectric lines (aka F waves). The atria in these regions are merely quivering and no longer beating.
Question
Which one of the following atrial arrhythmias is intensely irritable to the point where the atria are merely quivering and no longer beating?

a. Atrial flutter
b. Atrial fibrillation
c. Wandering pacemaker
d. Premature atrial contraction
Answer
b. Atrial fibrillation
Rationale
D. Rationale: Treatment for AF is determined by clinical presentation. Atrial fibrillation is treated pharmacologically, by ablation, or with a combination of both. Patients also undergo anticoagulation therapy for possible thrombus formation. The clinician may also consider controlling the heart rate pharmacologically and treating the rhythm with electro conversion. Corticosteroids, however, are not a pharmacologic treatment for AF.
Answer choice A – Cardioversion should be considered in patient in AF who are hemodynamically unstable.
Answer choice B – Calcium channel blockers, such as diltiazem, help control the heart rate in patients with atrial fibrillation.
Answer choice C – Digoxin are given to control the rate and rhythm in patients with atrial fibrillation.
Question
Which one of the following interventions is not used to treat atrial fibrillation?
a. Electro conversion
b. Calcium channel blockers
c. Digoxin
d. Corticosteroids
Answer
d. Corticosteroids