Dopamine in ACLS
Dopamine is a commonly used vasoactive medication in Advanced Cardiovascular Life Support (ACLS) for patients with bradycardia and hypotension. This article explains how dopamine works, its dose-dependent effects, indications in ACLS algorithms, safe administration considerations, and how to manage infusion changes to optimize patient outcomes.
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
- Dopamine is a pressor.
- It is indicated as a second choice for bradycardia and any algorithm with hypotension.
- The normal range is 2–20 mcg/minute, depending on the desired effects.
- The provider MUST be aware of the concentration of the dopamine infusion.
Dopamine is administered as a continuous infusion and exhibits dose-dependent effects based on the infusion rate. In ACLS, dosing typically ranges from 2 to 20 mcg/kg/min, depending on whether the clinical goal is to support heart rate, contractility, or blood pressure. For step-by-step dopamine drip calculations and infusion setup, see dopamine infusion calculation guide . Dopamine’s dosing range is between 2–20 mcg/kg/min.Dosing
Dopamine Dosing at 5–10 mcg/kg/min
Once we move to 5 mcg/kg/min and 10 mcg/kg/min, the mechanism of action is predominately beta1 (β1) in the heart. Five is a magic number with dopamine infusion, and we’ll talk more of it later. Beta increases the rate of heart contractility, which means dopamine acts as a positive chronotrope. Beta also increases the force of contractility, which means dopamine acts as a positive inotrope. Overall, when dopamine is administered between 5 and 10 mcg/kg/min, the effect is predominately beta.
Dopamine primarily stimulates beta receptors when administered between 5 and 10 mcg/kg/min.
Dopamine Dosing at 15–20 mcg/kg/min
We begin to see the alpha1 (α1) effect activate at the 15–20 mcg/kg/min range. The alpha effect is peripheral vasoconstriction in the vessels. Dopamine now acts as a vasopressor, causing vasoconstriction to raise the blood pressure.
The golden rule “fluids before pressors” now comes into play. If you are causing vasoconstriction and your patient is volume depleted, there is nothing to press. You can’t raise any blood pressure because there is nothing “in the tank.” Remember to give fluids before vasopressors.
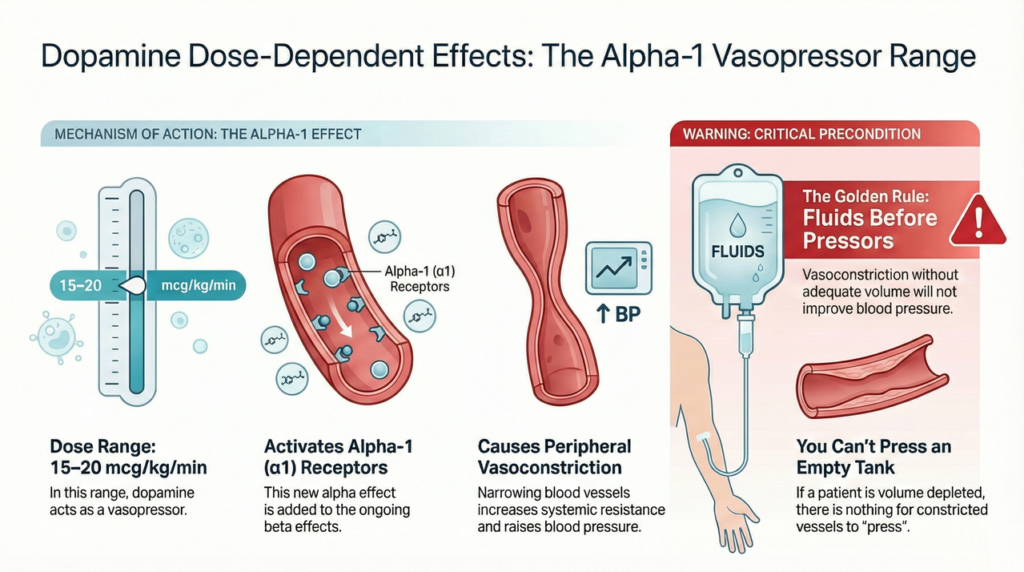
At doses of 15–20 mcg/kg/min, dopamine primarily stimulates alpha-1 receptors, causing peripheral vasoconstriction and increased blood pressure. Adequate volume resuscitation is essential before initiating vasopressor therapy.
Importantly, as we pass the 10 mcg/kg/min range, we are not lessening any of dopamine’s beta effects. We’re simply adding alpha effects.
Between 15 and 20 mcg/kg/min, dopamine stimulates alpha receptors, producing alpha effects.
Indications for Dopamine Use in ACLS
Dopamine is the second drug of choice in the ACLS bradycardia algorithm if atropine is ineffective. Remember, if you’re administering dopamine to raise the heart rate, you want those beta effects which occur somewhere between 5 and 10 mcg/kg/min.
Past that, you’ll move into alpha vasopressor effects, which may not raise the heart rate, especially in bradycardic patients because the problem is low heart rate. You’ll also find dopamine in any algorithm where hypotension is a factor.
Precautions and Contraindications
- Correct hypovolemia before starting dopamine, as vasoconstriction without adequate volume can worsen tissue perfusion.
- Use caution in patients with tachyarrhythmias, as dopamine may increase heart rate and myocardial oxygen demand.
- Monitor closely for extravasation, which can cause tissue necrosis.
- Avoid abrupt dose escalation, which may precipitate hypertension or arrhythmias.
- Use caution in patients with peripheral vascular disease due to vasoconstrictive effects at higher doses.
Dopamine Concentrations: What You Need to Know
Dopamine has varying concentration levels. It may be administered at 400 mg in 250 mL with a concentration of 1600 mcg/mL. Be careful in the ICU because some patients may be on an 800 mg per 250mL concentration of dopamine. These are often patients with heart failure, and they cannot tolerate that extra fluid. You must know the exact concentration before switching the patient over to your pumps for transport.
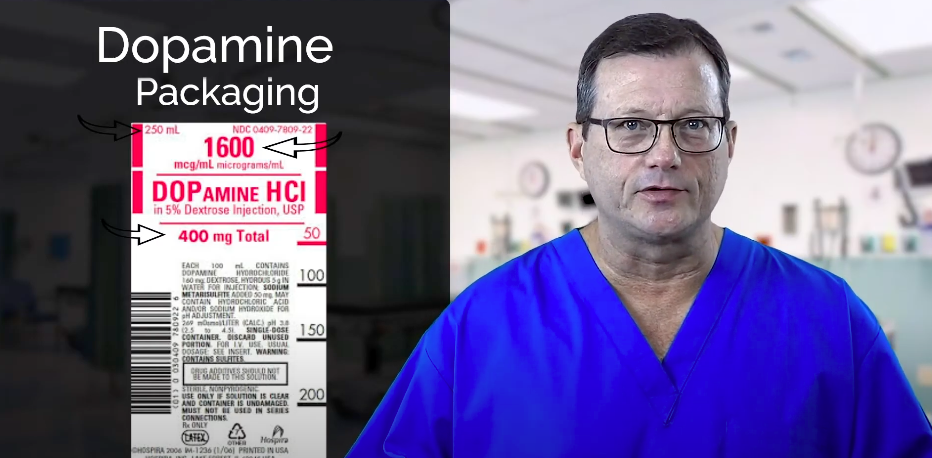
A dopamine concentration of 1600 mcg/mL.
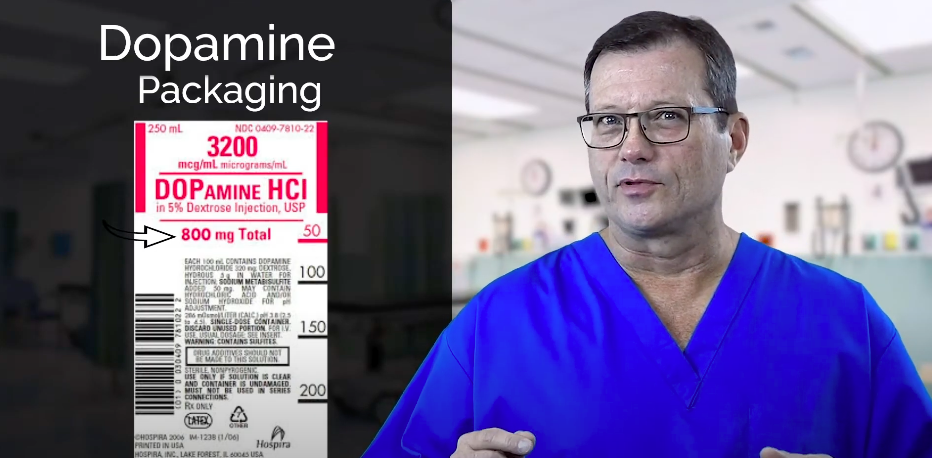
Dopamine concentration of 3200 mcg/mL, which may be used for patients with heart failure.
Tapering and Discontinuation
Dopamine infusions should be tapered gradually rather than stopped abruptly. Sudden discontinuation may lead to acute hypotension, reduced cardiac output, and clinical deterioration. When weaning dopamine, decrease the infusion rate slowly while monitoring blood pressure, heart rate, and overall perfusion. Ensure alternative hemodynamic support is in place if needed before discontinuing the medication completely.
Dopamine’s mechanism of action changes as the dose increases. At lower doses in the 5–10 mcg/kg/min range, you’ll see dopamine’s beta effects. At doses of 15–20 mcg/kg/min, you’ll also see its alpha effects. In ACLS, dopamine is considered only after atropine in ACLS has failed to resolve bradycardia. Physicians must know the exact concentration of dopamine a patient requires.Summary
More Free Resources to Keep You at Your Best
Editorial Note
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
More to Learn

Download the Pulseless electrical activity (PEA) and Asystole algorithm to learn the protocols / treatment of these nonshockable rhythms.
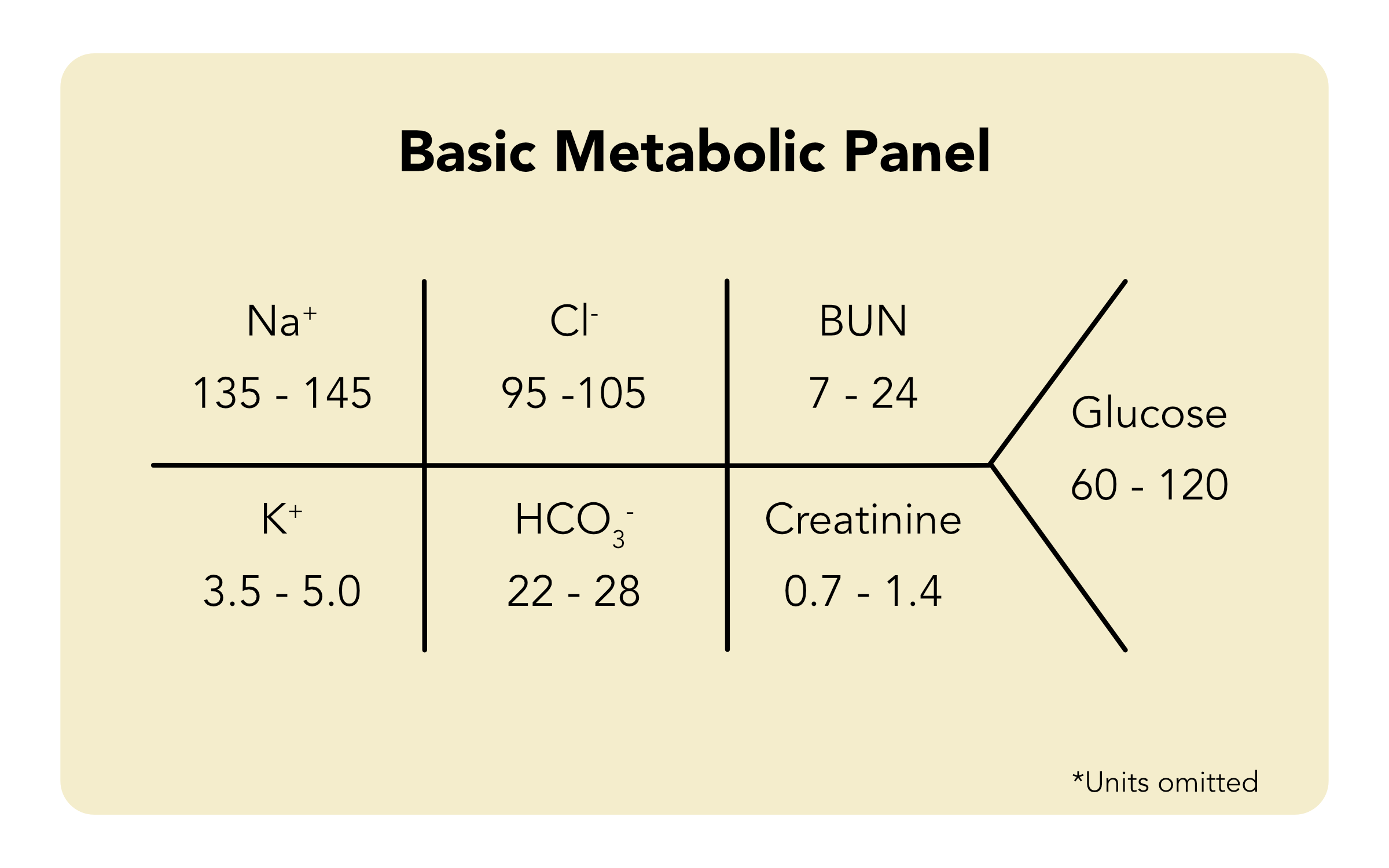
Read our detailed article and watch the video on Electrolytes. Learn about the imbalances of six types of electrolytes.