Arrhythmias Flashcard 1
Rationale
A. Rationale: The PALS guidelines recommend giving epinephrine IV at a dose of 0.01 mg/kg every 3 to 5 minutes, or as needed until the patient’s condition improves, for pediatric patients with AV block with persistent and symptomatic bradycardia despite adequate oxygenation, ventilation, and cardiopulmonary resuscitation.
Question
What is the pediatric dose of IV epinephrine for symptomatic AV block?
a. 0.01 mg/kg every 3–5 minutes
b. 0.02 mg/kg every 3–5 minutes
c. 0.05 mg/kg every 3–5 minutes
d. 0.08 mg/kg every 3–5 minutes
Answer
a. 0.01 mg/kg every 3–5 minutes
Rationale
C. Rationale: According to the PALS guidelines for tachycardia with a pulse, “the initial interventions in a child presenting with tachycardia are as follows: maintain a patent airway and assist breathing as needed. Administer oxygen if hypoxemic. Attach to a cardiac monitor and identify the rhythm. Monitor blood pressure and oximetry. Establish intravenous access. Do not delay therapy.” Maintaining a patent airway with adequate oxygenation and ventilation helps ensure that vital organs are perfused, especially in cases where perfusion is compromised.
Question
A 2-year-old girl presents with palpitations, dyspnea, irritability, and poor feeding. The assessment reveals a heart rate of 210 bpm. On arrival to the emergency department, she is noted to be pale with cyanotic lips. Physical examination also includes a respiratory rate of 37 breaths/minute with bilateral wheezes on auscultation of the lungs. The initial management for this patient is:
a. Monitor closely
b. Rapid defibrillation
c. Maintain a patent airway, assist breathing, ventilate, and oxygenate
d. Perform high-quality CPR
Answer
c. Maintain a patent airway, assist breathing, ventilate, and oxygenate
Rationale
C. Rationale: Since hypoxia is the most common cause of bradycardia in a child, the team should first establish a patent airway and assist breathing as needed with 100% oxygen. The team should quickly obtain intravenous or intraosseous access and perform 12-lead electrocardiography (ECG). Maintaining a patent airway with adequate oxygenation and ventilation helps ensure that vital organs are perfused, especially in cases where perfusion is compromised. If these interventions do not quicky improve the child, CPR with high quality chest compressions is initiated.
Question
A 7-year old female presents with a heart rate of 52 beats per minute and irregular. The child is lethargic. What is the initial intervention in a child presenting with symptomatic bradycardia?
a. Monitor closely
b. Give atropine
c. Maintain patent airway, assist breathing, ventilate, and oxygenate
d. Perform high-quality cardiopulmonary resuscitation (CPR)
Answer
c. Maintain patent airway, assist breathing, ventilate, and oxygenate
Rationale
C. Rationale: This is a second-degree AV block, or Mobitz type II. Impulses from below the AV node within the Purkinje system are blocked. On 12-lead ECG, the tracing shows a fixed PR interval (no progression or lengthening) with intermittent dropped beats. This type of AV block causes symptoms.
Question
A child with symptomatic bradycardic rhythm is treated in the ED. Identify the rhythm.

a. Sinus bradycardia
b. First-degree AV block
c. Second-degree AV block
d. Junctional rhythm
Answer
c. Second-degree AV block
Rationale
C. Rationale: Synchronized cardioversion is indicated in patients with supraventricular tachycardia with a pulse who remain unresponsive to medication and are deteriorating hemodynamically. Synchronized cardioversion delivers energy or shock in coordination with the R wave. It is important to note that the delivery of the shock is timed with the R-wave. Otherwise, the shock may be delivered during the vulnerable T waves, converting SVT to VF. Synchronized cardioversion is a painful procedure, and thus sedating the patient is recommended.
Question
A patient in SVT is unresponsive to vagal maneuvers and adenosine. She remains in tachycardia, with weak pulses. She is increasingly lethargic, cyanotic, and in respiratory distress. The most appropriate intervention for this child is:
a. Close monitoring
b. To apply a vagal maneuver
c. Synchronized cardioversion
d. Rapid defibrillation
Answer
c. Synchronized cardioversion
Rationale
B. Rationale: Supraventricular tachycardia (SVT) is caused by aberrant impulses coming from random areas in the ventricles. These impulses reenter within the atrioventricular node or through an accessory pathway, generating additional aberrant impulses. On the 12-lead ECG, SVT is seen as a regularly occurring narrow QRS complex with no discernible P waves. The P waves are either buried within the QRS complex or seen before or right after it, distorting the morphology. SVT is sudden in its onset and termination.
Question
A patient is brought to the ED with dyspnea and palpitations with a heart rate of 210 bpm. She is hooked to a 12-lead electrocardiogram and shows the following tracing. What is the rhythm?

a. Sinus tachycardia
b. Supraventricular tachycardia
c. Ventricular fibrillation
d. Ventricular tachycardia
Answer
b. Supraventricular tachycardia
Rationale
D. Rationale: Pediatric patients with a cardiac condition that produces an arrhythmia are at risk for developing cardiac arrest rhythms such as ventricular fibrillation or pulseless electrical activity while performing strenuous activities. Therefore, athletic departments require coaches and other personnel present in athletic events to be trained in BLS and provide emergency equipment to be used when needed in sports events.
Question
A pediatric patient with congenital cardiac arrhythmias will likely exacerbate their condition and may progress to cardiac arrest when:
a. Discontinuing their medications
b. Acutely ill with a viral infection
c. Becoming dehydrated
d. Performing strenuous sports activities
Answer
d. Performing strenuous sports activities
Rationale
A. Rationale: Bradycardia in children is a heart rate that is less than 60 beats per minute. Bradycardia is an indication that a child is critically ill. Older children may have a HR < 60 bpm during sleep, especially if they are athletes.
Question
Bradycardia in pediatric patients presents with a heart rate of:
a. Less than 60 beats per minute
b. 60 to 90 beats per minute
c. 100 to 120 beats per minute
d. 120 beats per minute and higher
Answer
a. Less than 60 beats per minute
Rationale
A. Rationale: Torsade’s de pointes is a form of polymorphic ventricular tachycardia occurring in the context of a prolonged QT interval. It is characterized in the 12-lead ECG as a rapid, irregular QRS complex that twists around the isoelectric line at a rate of about 200–250 bpm. This tachyarrhythmia occurs in bursts and then resolves spontaneously, or it may develop into VF, causing significant hemodynamic compromise and even death. To diagnose torsade’s de pointes, the patient must have evidence of both paroxysmal ventricular tachycardia and a prolonged QT interval.
Question
Identify the following rhythm:

a. Torsade’s de pointes
b. Atrial fibrillation
c. Ventricular flutter
d. Atrial flutter
Answer
a. Torsade’s de pointes
Rationale
D. Rationale: This 12-lead electrocardiogram depicts atrial flutter. There is a reentrant circuit in an atrial flutter that causes a repeated loop that depolarizes the atrium. Because of these reentries, not all the P waves conduct a circuit through the AV node, resulting in a much faster atrial rate than the ventricular rate. The atrium beats at a rate of 250–350 beats per minute, while the ventricular rate is about 150 beats per minute. The P waves that reenter and don’t conduct through the AV node cause the sawtooth appearance on ECG characteristically seen in atrial flutter.
Question
Identify the rhythm of this 12-lead electrocardiogram tracing.
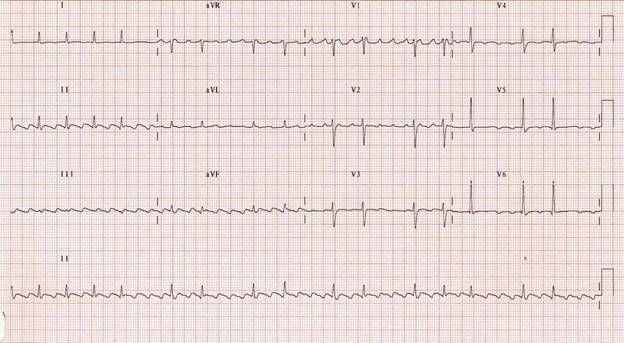
a. Torsade de pointes
b. Atrial fibrillation
c. Ventricular flutter
d. Atrial flutter
Answer
d. Atrial flutter