Pacemaker Changes Flashcard
Rationale
B. Rationale: Undersensing produces multiple small spikes on ECG during motion or ambulation while recording the ECG. These spikes are produced by movement of the muscles. There are also absent pacemaker spikes, and ventricular asystole may be produced. Oversensing is produced during strenuous exercise, especially in younger individuals.
Question
A 54-year-old man who is dependent on a pacemaker was chopping wood when he had a sudden episode of syncope. Which pacemaker abnormality erroneously stimulates the heart and causes syncope?
a. Loss of battery voltage
b. Undersensing
c. Oversensing
d. Failure to capture
Answer
b. Undersensing
Rationale
C. Rationale: In a one-chamber pacemaker, the artificial impulse is stimulated over the right ventricle. So the right ventricle is activated first, then the left ventricle over the septum. There will be a delayed impulse over the left septum, and this will produce a left bundle-branch block pattern on ECG. If the electrode was placed on the left ventricle, then a right bundle-branch pattern will be seen on ECG.
Answer choice A – Oversensing would result in an inadequate number of pacer spikes despite the patient’s low intrinsic heart rate.
Answer choice B – Undersensing would result in multiple unnecessary pacer spikes despite the patient’s intrinsic heart rate.
Answer choice D – If the pacemaker electrode were placed over the left atrium, a right bundle branch pattern would result.
Question
A 64-year-old man with a one-chamber pacemaker has a 12-lead ECG tracing that shows a left bundle branch block pattern. What could have caused this configuration?
a. This is a sign of pacemaker oversensing.
b. This is a sign of pacemaker undersensing.
c. The electrode of the pacemaker is placed on the right atrium.
d. The electrode of the pacemaker is placed on the left atrium.
Answer
c. The electrode of the pacemaker is placed on the right atrium.
Rationale
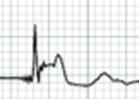
C. Rationale: The ECG spike at the beginning of the ECG tracing refers to the stimulus from a one-chamber pacemaker. This spike is a must-know configuration and can only be produced by a pacemaker. The pattern will also depend on the impulses influenced by the pacemaker and the spontaneous impulses produced in the heart.
Answer choice A – Myocardial ischemia would manifest as ST depression.
Answer choice B – Myocardial infarction would manifest as ST elevation.
Answer choice D – Wolf-Parkinson-White syndrome is a rapid dysrhythmia that displays a characteristic delta wave on ECG.
Question
How do you interpret this ECG tracing?
a. Myocardial ischemia
b. Myocardial infarction
c. A paced rhythm
d. Wolff-Parkinson-White syndrome
Answer
c. A paced rhythm
Rationale
C. Rationale: Cardiac pacing is indicated for patients with medically refractory and symptomatic hypertrophic obstructive cardiomyopathy. Dual-chamber pacing improves the symptoms in these patients by lowering the left ventricular outflow tract gradients. This is done by forcing the right ventricular pacing to move the ventricular septum to the right ventricle during systole, which results in a widening of the left ventricular outflow tract.
Question
Which of the following effects of a dual-chamber pacemaker relieves the patient from the symptoms of severe hypertrophic obstructive cardiomyopathy?
a. Synchronizes its impulses with the sinoatrial impulse to prevent palpitations
b. Provides a positive inotropic effect on the ventricles
c. Lowers the left ventricular outflow tract gradients
d. Provides a positive chronotropic effect on the ventricles
Answer
c. Lowers the left ventricular outflow tract gradients
Rationale
D. Rationale: Complete atrioventricular blocks and diseases involving sinus node dysfunction are the most frequent reasons for providing patients with chronic pacing. This patient population is responsible for about 40% of all pacemaker implantations. Other indications for pacemaker placement include bradycardia, atrial fibrillation, bifascicular blocks, and incomplete trifascicular blocks. Second-degree AV block, sick sinus syndrome, long QT interval syndromes, sleep apnea, hypertrophic obstructive cardiomyopathy, and heart failure with wide QRS complexes are also indications for pacemaker implantation.
Answer choice A – Occlusion of the left anterior descending artery will not affect the SA node and lead to the need for a pacemaker.
Answer choice B – Paroxysmal supraventricular tachycardia is not an indication for a pacemaker. It begins abruptly and ends without intervention.
Answer choice C – A history of atrial fibrillation is not an indication for a pacemaker.
Question
Which one of the following patients needs a pacemaker?
a. A patient with coronary artery disease with a 100% occlusion of the distal left anterior descending artery
b. A patient who went into a symptomatic paroxysmal supraventricular tachycardia
c. A patient with a history of atrial fibrillation
d. A patient with complete atrioventricular block
Answer
d. A patient with complete atrioventricular block
Rationale
B. Rationale: Undersensing is dangerous. A spike that falls on a vulnerable period, such as on a T phenomenon, can induce ventricular fibrillation. This has been documented, although very rarely, and is usually seen in patients with severe ischemia. Undersensing can be avoided if the threshold is set at a lower voltage, typically 1.5–2.5mV.
Question
Why is a pacemaker usually set at a low voltage of 1.5–2.5 mV?
a. To prevent oversensing
b. To prevent undersensing
c. To prolong battery life
d. This is the maximum capacity of the pacemaker battery
Answer
b. To prevent undersensing